Case Study

Mexico City's ProAire programme
26th February, 2016
The initiative
On 27 April 2010 in Freetown, the president of Sierra Leone, Ernest Bai Koroma, launched “free health care for children under 5 and for pregnant and breastfeeding women”, the Free Health Care Initiative (FHCI). [3] This followed an announcement of the policy at the UN in the preceding year, as part of his government’s to further the aims of the country’s Health Sector Strategic Plan and its Poverty Reduction Strategy Paper (PRSP II), in line with the UN’s Millennium Development Goals, principally numbers 4 (reduce child mortality) and 5 (improve maternal health).The challenge
For many years Sierra Leone was in last place in the UN Development Programme's Human Development Index because of its poor health indicators. [1] In 2000, there were 1,800 mothers dying for every 100,000 live births and 286 children under five dying for every 1,000 live births, the highest global levels globally. Mother and child mortality rates were unacceptably high, due largely to poor healthcare services and difficulties in accessing and using those services.
Sierra Leonians' limited use of their healthcare services was due to a number of factors which affected the entire health system, including:
The public impact
By 2015, there had been significant improvements in the indicators in the World Health Index [4]:
According to government figures, the investment in medical care for under-fives had more than doubled.
Stakeholder engagement
The UK Department for International Development (DFID) provided Sierra Leone with extensive support for the initiative in the following ways:
There was additional funding for the programme from government of Sierra Leone (12%), the Africa Development Bank, the World Bank, the UN agencies UNPFA and UNICEF, and the UN Foundation's Global Fund. The government, with the help of international partners, bought US$ 10 million dollars of drugs and supplies and distributed them across country's health centres. Financing was primarily for payment of health workers' salaries (52%), drugs and consumables (40%) and service delivery activities (8%).
In preparation for the FHCI launch, six technical working groups designed the reforms and changes in the health system necessary to ensure the smooth running of the FHCI's roll-out.
Political commitment
President Bai Koroma was strongly committed to making the policy effective and the initiative was a high government priority. As he said at the launch: “I want to reassure the nation that I am determined to make this policy work. You may have heard hollow promises from politicians before about free services, but in the past these announcements have not been backed up by other actions. This time it will be different.” [6] He led the reform process and had toured the country to check that hospitals and health centres were prepared for the launch day. The government’s financial investment in the FHCI provided a tangible demonstration of its commitment.Public confidence
President Bai Koroma’s job approval rating was 85% in 2008, which shows high public confidence in the government. [7] However, there is limited information about public confidence in the healthcare policy itself.Clarity of objectives
The objectives to reduce maternal and child mortality rates and to improve general health indicators were clear when stated at the outset and could be measured by an authoritative external source.Strength of evidence
Information on study or pilots conducted could not be found. In addition to this, the FHCI was the first such initiative ever implemented in Sierra Leone and there was no information whether the idea was taken from similar existing systems, such as the UK's National Health Service.
According to President Bai Koroma: “last September when I visited the United Nations General Assembly, I announced our new free health care policy at a meeting chaired by the UK prime minister and the president of the World Bank. Five other heads of state also announced that they would be extending their free healthcare policies. But we in Sierra Leone will be the first to make this happen."
Feasibility
In addition to this, UNICEF data on cost feasibility of the project shows that the FHCI is heavily dependent on donor funds and that it would require substantial budget and donor investments over the next four years for its successful implementation. Hence it has been rated as fair.
In November 2009, during planning for the FHCI, human resources for health (HRH) was picked out as an area needing immediate attention. However, according to UNICEF data, the number of health staff is still insufficient to meet the demand for service delivery, although it has increased significantly since the launch of the FHCI.
The FHCI is heavily dependent on donor funds, given that the government of Sierra Leone provided only 12% at the launch. In 2011, UNICEF stated that the continued success of the FHCI would depend on substantial budget and donor investments and the maintenance of donor enthusiasm.
Management
The government employed ‘maternal health promoters' (MHPs) with experience in providing assistance during pregnancy, labour and birth to manage the individual prenatal, natal and postnatal care. Their major responsibilities were to support women during pregnancy, refer them to health centres for delivery, and assist them with advice on breast-feeding and general health issues following the birth. Training sessions were organised by Health Poverty Action for the MHPs.
In addition to this, the government doubled the health workers' salaries (partly to combat corruption) and established an attendance monitoring system for health workers, run by the Ministry of Health and Sanitation with DFID's involvement. It recorded the daily attendance of all health sector employees, penalised unauthorised absences, and removed inactive staff from the payroll. This monitoring system had immediate effects on staff discipline. [9]
Measurement
There were measurable and annually measured external indicators (for instance the UN maternal and under-five mortality rates) to capture the outcomes of the policy. However, here was no established, effective internal system to monitor and measure the impact of the FHCI consistently. As a result, implementation and accountability were major challenges. For example, women described how they were sent to private pharmacies to buy drugs and were told that drugs and consumables were available but only for sale, despite its being a free healthcare initiative. While healthcare workers and government officials knew about such problems, there was very little chance of specific instances being identified and addressed.Alignment
There was effective coordination between the government and UNICEF in providing procurement support for the initiative. Further there was excellent collaboration between the government, its development partners, NGOs, civil society groups and UN agencies. The Ministry of Health and Sanitation had an important partnership with DFID as the attendance monitoring system (in which the Global Fund was also involved serves to indicate.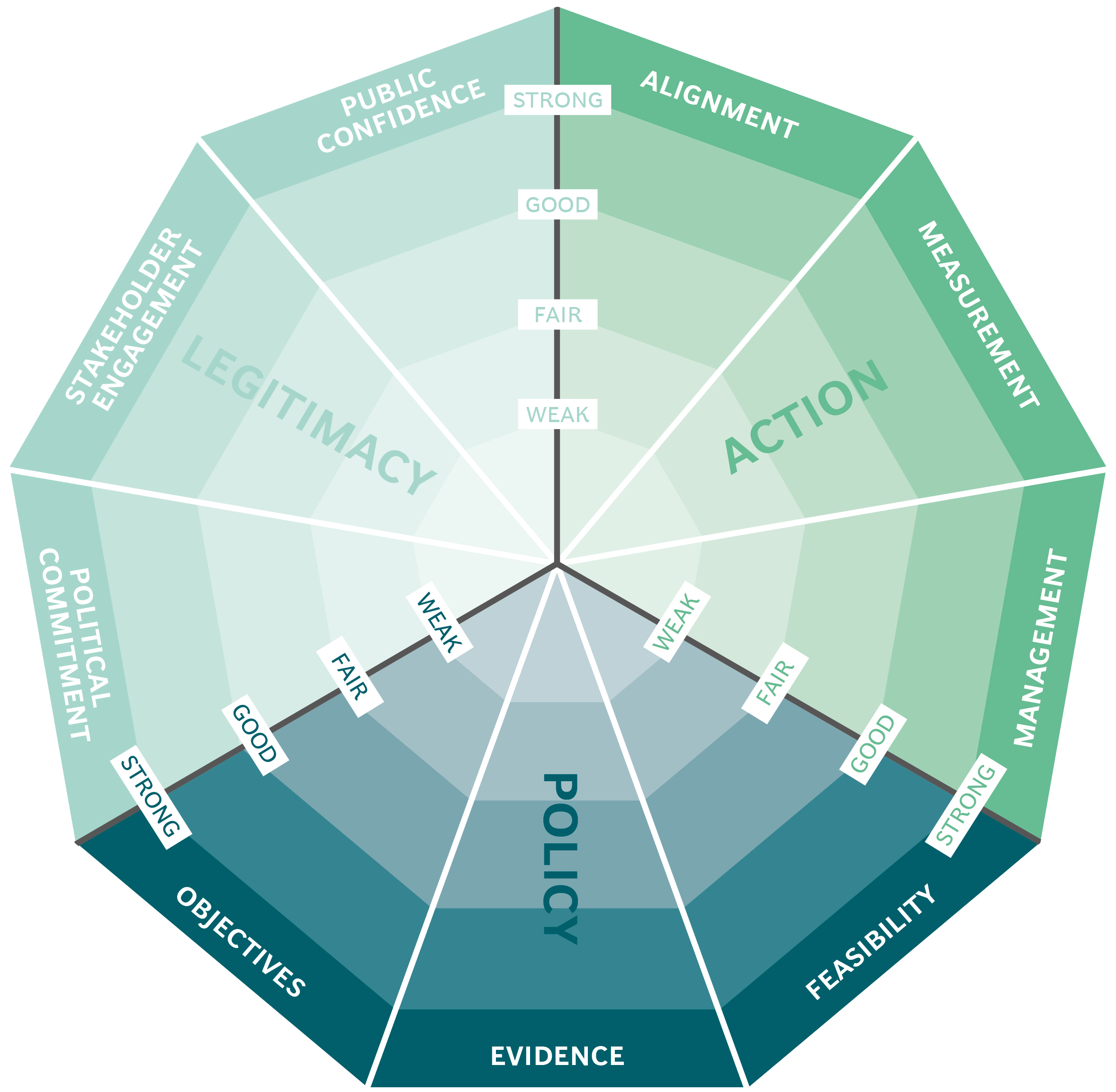
This case study has been assessed using the Public Impact Fundamentals, a simple framework and practical tool to help you assess your public policies and ensure the three fundamentals - Legitimacy, Policy and Action are embedded in them.
Learn more about the Fundamentals and how you can use them to access your own policies and initiatives.