Case Study

Mexico City's ProAire programme
26th February, 2016
The initiative
In order to address the risks to the health of women and children and the rapid population growth, the government's objectives were to increase the use of contraceptives among women and, following on from this objective, to reduce fertility rates of women in rural areas. To achieve these goals, the government partnered with the International Centre for Diarrheal Disease Research, Bangladesh (ICDDR,B). In 1977, the ICDDR,B introduced an experimental maternal and child health and family planning programme in 70 villages in Bangladesh. From this experimental programme came the Family Planning and Health Services Project (FPHSP).
The FPHSP recruited literate young married women as outreach workers, most of whom were members of influential families in the villages in which they were to work. The outreach workers visited all the married women of childbearing age in their village once a fortnight to give them advice about the women's contraceptive needs and encourage them to adopt contraceptive measures.
The health workers provided those women who were considering adopting family planning methods with a choice of pills, foam tablets and an injectable contraceptive. They also encouraged the women who expressed an interest in IUD services to visit a nearby clinic. In addition to this, the government used mass media to stimulate a change in attitudes to family size.
The challenge
About 40 years ago, a Bangladeshi woman had, on average, more than six children. This very high fertility rate, together with poor nutrition and lack of access to quality health services, jeopardised the health of women and their children. High fertility rates also had a much wider impact: rapid population growth “represented a major constraint on the country’s economic development and social progress”.[1]The public impact
In the treatment area, the use of modern contraceptive methods rose from 7 percent to 20 percent of married women of reproductive age within three months and to over 30 percent after a year and a half. At a national level, the use of contraceptives in 1985 had reached 45 percent and by 2004 it had increased to 60 percent. The fertility in the country overall was reduced from an average of more than six children per woman in 1975 to slightly more than two in 2015.
An indirect impact was that the project improved the status of women by raising the levels of knowledge about family planning, increasing the access to family planning services, and challenging prevailing beliefs that large families were best.
Stakeholder engagement
The major project stakeholders were key ministries within the government, the ICDDR,B and the health workers they recruited for the project. These stakeholders supported the initiative as they believed in the need for Bangladesh to address high fertility rates. To engage local health workers, whose buy-in was fundamental to achieving impact, the ICDDR,B offered training sessions and supervisory support. Over a period of six weeks of intensive training, female health workers learned about contraception, field visit methods, and maternal and children’s health.Political commitment
The objectives of reducing population growth were very high up on the Bangladesh government’s agenda at the time: the government, therefore, allocated its managerial talent as well as a sizeable share of its budget, almost six percent of the government’s development budget, to the programme.Public confidence
Most villagers were already familiar with and appreciative of the ICDDR,B. Due to its previous role in leading an initiative that helped to reduce diarrheal mortality in the area, the ICDDR,B enjoyed high levels of trust as an institution. The recruitment of local female health workers also helped to build public support for the initiative.[2] The government’s decision to partner with the ICDDR,B was therefore a key driver of public confidence.Clarity of objectives
The main objective was to send trained female workers into the villages to educate people and bring about an increase in the use of contraceptives, along with a reduction in fertility rates. These objectives were maintained throughout the initiative.Strength of evidence
The idea of the programme was derived from a similar project initiated by ICDDR,B in 1975 called the Matlab project. The ICDDR,B had identified the causes of the failure of that project – using “largely illiterate, elderly female workers”,[3] few of whom “had practised contraception themselves”. To address these programmatic weaknesses, the ICDDR,B selected a different kind of health worker: also female, but young and literate and with experience of using contraception.Feasibility
Concern about finance was a major issue at the start of the implementation of the policy in 1977, due to the high costs incurred by the programme and the limited funding available at the beginning. One important limitation was the cost of the project. The total cost that incurred for rolling out the policy between 1978 and 1985 was about three times as high as the cost that incurred in the sample villages of the comparison area. [4]
It is important to note that at a later stage, the programme was able to secure funding from large international organisations, such as USAID, UNDP, and especially the World Bank.[5] However, this was a result of its success and not foreseeable at the outset of the initiative.
Management
Project staff were recruited and trained effectively, with local supervisors providing all relevant information:
According to a number of reviews, the central management of the programme led to some inefficiencies at the operational and funding level. Programme enhancements, for example, were not implemented efficiently.[6]
Measurement
Two metrics were used to gauge the effectiveness of the project: cost-effectiveness and a comparison of contraceptive use and fertility rates in the treatment area with that of sample villages outside the treatment area. The measurement process included the following aspects:
Alignment
To meet the objectives, the programme had mechanisms in place to ensure effective coordination between the key actors. As a result, an alignment of interests was constantly maintained: the authorities, the organisational staff, and the local public were well coordinated and well equipped to achieve the programme’s objectives. There was also close alignment within the project teams: the organisation of the project promoted internal cohesion among staff members of the same level as well as of different levels.Bibliography
CASE 13: Reducing fertility in Bangladesh, Center for Global Development
Community-Based Distribution of DMPA: The Matlab Project, Bangladesh, 2007, K4Health
Family Planning Success Stories in Bangladesh and India, Moni Nag, November 1992, The World Bank
The World Bank and the Bangladesh Population Program, 1991, World Bank Group
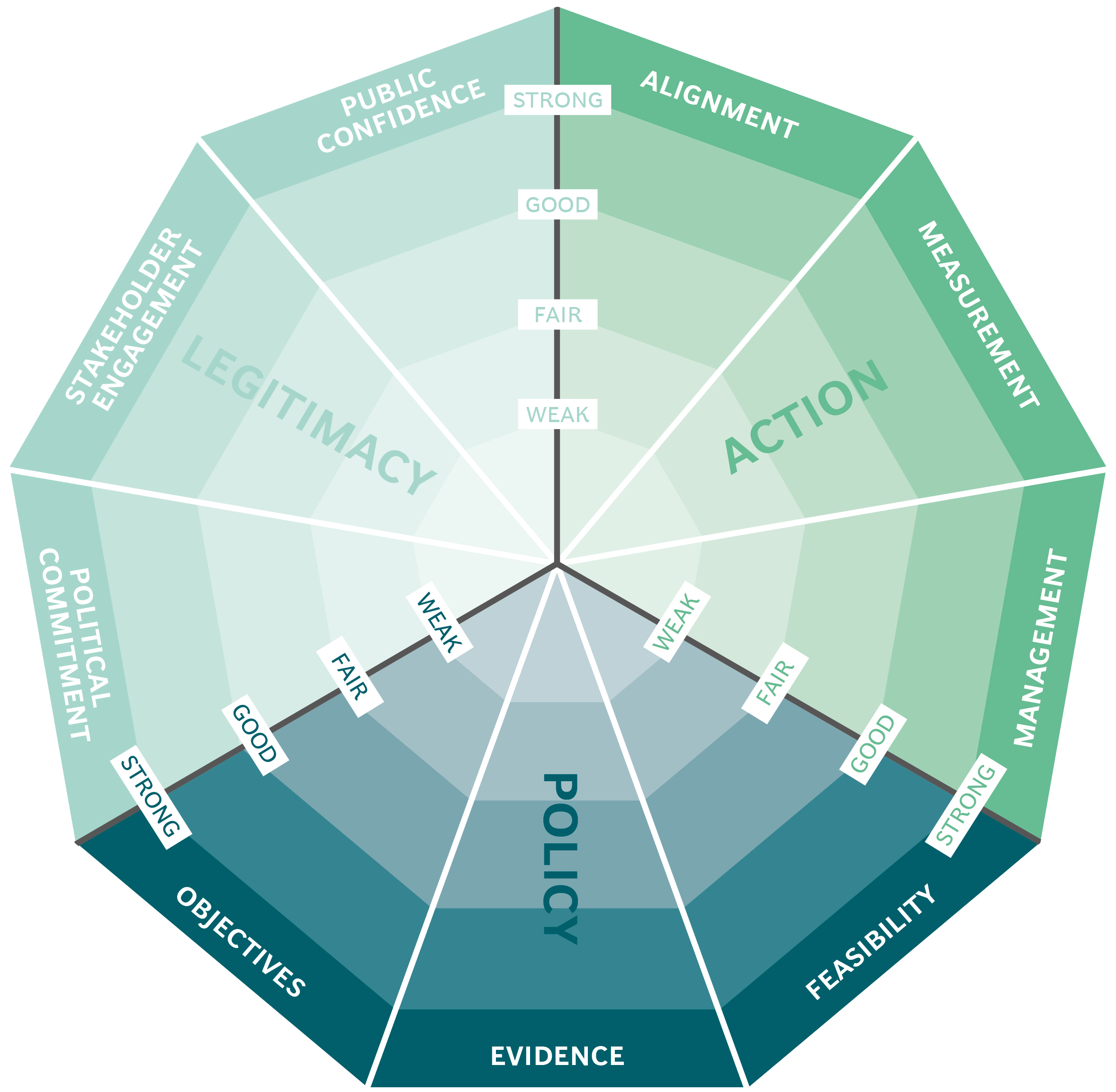
This case study has been assessed using the Public Impact Fundamentals, a simple framework and practical tool to help you assess your public policies and ensure the three fundamentals - Legitimacy, Policy and Action are embedded in them.
Learn more about the Fundamentals and how you can use them to access your own policies and initiatives.